

As a member of the marketing team at HonorBridge, I’ve watched countless visitors pass through our Chapel Hill facility, admiring its modern design and donor-inspired art installations. They pause to read the stories of recipients and donors on our donor wall and take a peek inside the large conference rooms, but often the double doors to the Donor Care Center go completely unnoticed. Ironic, really, as these doors open to the most impressive and essential space in the entire building.
“Through those double doors is our Donor Care Center (DCC), where we recover organs and tissues from donors onsite,” I explain during tours. It always takes a few moments for them to grasp my meaning, but once they do, the questions come flooding in.
“There are donors back there right now?”
“Is this like a hospital?”
“There is a MORGUE back there?!”
Yes, yes, and, well … yes.
The DCC is a state-of-the-art medical facility, much like a small hospital, that allows us to recover organs and tissues for transplantation without relying on overcrowded transplant hospitals. This space includes our Donor Care Unit (DCU), where donors are brought, cared for, and prepped by our nursing team before surgery. From there, they move to our operating room, where a team of surgeons recover the organs and tissues that will save and heal lives.
A Unique Facility

“There are 24 organ procurement organizations (OPOs) that have donor care units, but only 11 have freestanding donor care units like this one,” says Jenn Buchanan, DCU manager. “We transfer adult brain dead donors from non-transplant hospitals who meet specific criteria. We have transferred from a transplant center under very specific circumstances, but I would say that is definitely not the norm.”
The ability to recover organs and tissues at our own location, without overcrowding existing transplant hospitals, has led to reduced costs, more gifts recovered, and more lives saved.
“According to the data, organs transplanted per donor in the DCU is higher compared to donors not transferred to the DCU,” says Jenn. “I think there could be a few factors in that, but one of them is that we only have one patient/donor to focus on, so we are able to jump right into developing a customized plan of care for that donor. I think we are able to prioritize the donor and their family without any other competing priorities.”
From Arrival to Recovery:
The Donor’s Journey

So, what exactly happens behind those double doors?
“Before a donor ever arrives at HonorBridge, so much work has already happened,” says Jenn. “Our team reviews the donor’s medical history, confirms with our medical directors that transfer is safe, coordinates with critical care transport teams, and ensures all staff and resources are ready. When the donor arrives, we transfer them to our equipment, receive updates from the transport team, perform a full physical assessment, and draw initial labs, all within the first 30 minutes.
From there, we present a customized plan of care, designed to honor the donor’s gift and maximize the number of organs available for transplant. This plan can include ventilator adjustments, procedures to improve organ function, or other targeted interventions. Every case is unique, and we continually adjust our approach based on how the donor responds.”
The ability to recover organs and tissues at our own location, without overcrowding existing transplant hospitals, has led to reduced costs, more gifts recovered, and more lives saved.
“According to the data, organs transplanted per donor in the DCU is higher compared to donors not transferred to the DCU,” says Jenn. “I think there could be a few factors in that, but one of them is that we only have one patient/donor to focus on, so we are able to jump right into developing a customized plan of care for that donor. I think we are able to prioritize the donor and their family without any other competing priorities.”
A Place for Families, Too


Families are welcome to visit once their loved one is settled, usually two at a time, accompanied by a Family Support Specialist. Because the DCU typically cares for just one donor at a time, each donor family receives personalized attention.
“They’re often invited to come sit at the bedside and we’re able to talk to them about what we’re doing,” says Jenn. “We bring chairs in, we let them sit and put the bedrails down so they can hold their loved one’s hand. We had one family who really wanted to wash their loved one’s hair, so we actually brought in a hairdresser and we helped facilitate that. We had a family that really wanted to play some music for their loved one, so we used our Alexa to do that for them.”
While families are asked to say goodbye right before the donor is rolled back into the operating room, they are always invited to stay in the family resource area during the process of recovery or find comfort outside in the adjacent Honor Garden, featuring a one-of-a-kind art installation as a tribute to individual donors.
In the DCU, donors and their families always come first, because without their generosity, none of this would be possible.
Imaging & Insight

CT imaging plays a vital role in the Donor Care Unit (DCU), thanks to the expertise of Kyle VanDePerre, HonorBridge’s CT technologist. With years of experience, Kyle has helped develop protocols that give surgical teams a clearer picture of each donor’s anatomy.
- Fast access: The CT scanner is just steps from the care area, allowing instant scans after procedures like bronchoscopy.
- Full focus on donors: Unlike in hospitals, the DCU’s equipment is dedicated solely to donor care, without competing for space or staff.
- 3D organ views: Detailed images help surgeons see vessels and anatomy before surgery, guiding the safest approach.
- Specialist support: CT and biopsy results are sent to transplant-trained experts virtually for quick, informed decisions.
Speed matters: Biopsy results are often ready in under an hour, keeping the recovery process moving. This efficiency, along with tools like kidney pumps that keep organs healthy until transplant, means more organs can be recovered and more lives can be saved.
The Process of Organ & Tissue Recovery

At HonorBridge, organ recovery often involves a mix of in-house and local surgeons. For example, some surgeons work at a hospital but have a contract with HonorBridge to perform local recoveries when needed (when a transplant center in another state can’t send their own surgeon, for example).
Some surgeons are HonorBridge employees and can perform recoveries directly. This helps speed up the process and saves transplant centers from sending a team. While heart and lung transplants usually require the recipient’s own surgical team to travel, abdominal organs like kidneys, liver, and pancreas are often recovered locally.

Timing is critical. Surgeons flying in are asked to arrive at least an hour before the scheduled surgery, or “cut time.” In the DCU, cut time means the moment surgery begins. The donor is brought to the operating room 45 minutes before that, prepared, and draped so that when the surgeons arrive, they can sign the necessary paperwork and begin right away. They also have access to a nearby lounge and locker rooms before surgery.
If there is a delay — for example, while awaiting liver biopsy results — surgeons can wait comfortably in the surgeon’s lounge. Members of their teams who are only needed for specific parts of the process, such as pumping at the end, also benefit from being close by without having to wait in the operating room.
The Room Where it Happens


The DCC’s operating room is designed exclusively for organ and tissue recovery, unlike a hospital OR, which handles a wide range of procedures. Needed equipment is always on hand, or can be quickly acquired, without the delays common in hospital systems.
One of the OR’s most exciting features is the new Teledoc camera system, nicknamed “Fancy Nancy” after our medical director, Dr. Nancy Knudsen, which allows medical directors or accepting transplant centers to remotely view procedures in real time. HonorBridge is proud to be the first OPO to pilot the use of a TeleDoc system in a donor care center.
“It’s like having a physician at your fingertips,” says Jenn. “Sometimes accepting transplant centers will say they will accept the liver pending visualization—so, instead of leaning over and trying to take pictures with cellphones, we can actually dial them into the Teledoc. We send them a secure link, and they are able to visualize for themselves. It’s moveable, so we can move it from room to room. We use it in recovery, we use it for training, we use it when the donors are here and we need a critical consult. It’s been great!”
What Happens After

After organ recovery, the donor’s body is closed up and returned to the on-site morgue. If they are a tissue donor, the tissue team will eventually bring the donor into the tissue suite, where they have their own separate prep room.
If they are not a tissue donor, the HonorBridge team will set up transportation to return the body to the funeral home, the hospital, the medical examiner, or wherever they need to go next. Out of respect, an HonorBridge team member always stays with the body until transfer is complete.
Opportunities for Growth
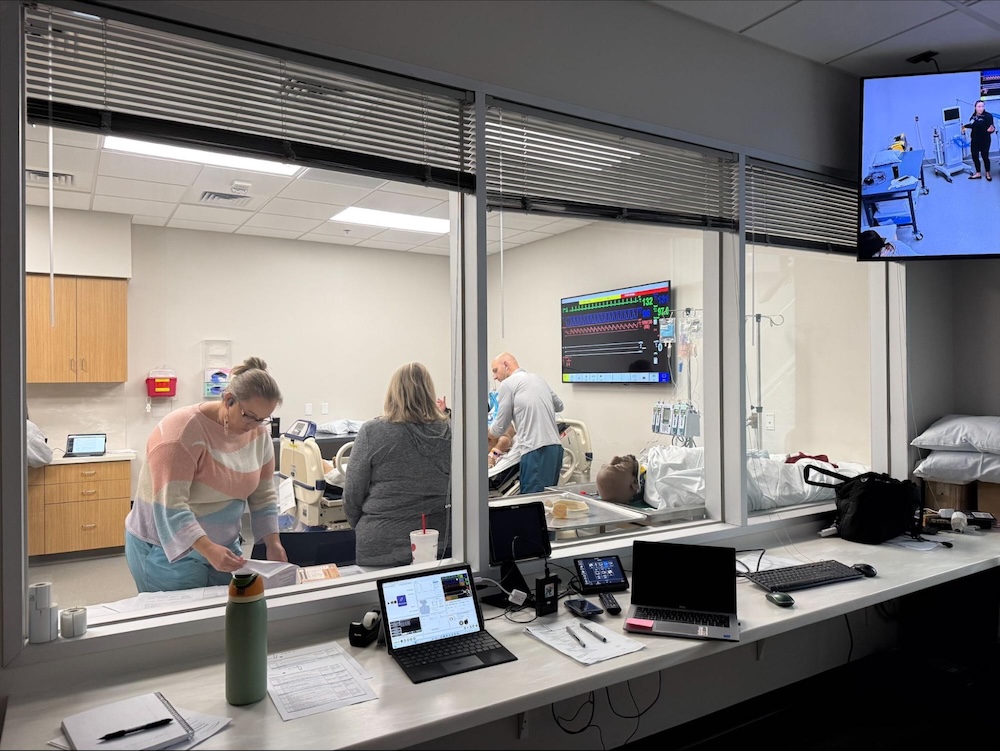

The DCC offers a simulation lab, which provides opportunities for clinical teams to hone their skills and share their knowledge with community partners. It also provides invaluable interdisciplinary opportunities for training and collaboration with other organ procurement organizations (OPOs), allowing teams to share best practices and learn from one another. An advanced audio-visual system allows training staff to record presentations to share with partners and new hires, and the adjacent observation room is perfect for small group training onsite.
One of the most exciting additions to the sim lab is a high-tech mannequin, one of the newest and most advanced patient simulators on the market.
“We bought one of the first 10 in the entire world,” says Jen. “For our team, realistic looking mannequins are great, but what they really need is for them to perform realistically. That’s what this new mannequin does. We can use him to train our staff for how to handle brain dead donors and DCD (donation after circulatory death) donors. You can change the lung sounds that you hear, you can change the heart sounds that you hear, we can even simulate different types of lung diseases because we can change the resistance. It is designed to connect to a ventilator and provide realistic pressure feedback, mimicking conditions such as pneumonia or other chest complications—teaching our team to assess and make decisions based on real world data.”
The mannequin also includes simulation software that allows for scenario creation. For example, a simulation can begin with a stable patient whose heart rate suddenly changes, prompting the team to respond appropriately. The mannequin also supports a wide range of procedures including chest compressions, IV insertions, catheter placements, surgical airways, intubations, and bronchoscopies—you name it!
More than a Building

If you visit the HonorBridge website, our mission is outlined on our “About Us” page: “We are devoted to building connections that save and heal lives through organ and tissue donation.” Since its opening in early 2024, the DCC has been instrumental in helping the organization do just that—but for those who work behind the double doors, it feels a bit more personal.
“Our mission is to give our full attention to the donor that is here,” says Jenn. “It’s such a gift that that family and that person has given to us, and to the people that they’re going to help and heal, that we all just come with such a sense of purpose and honor. Our goal is to provide compassionate, customized care to both the donor and the family. We want this to be as good of an experience as it can possibly be, knowing that this is the hardest time of their lives. My team is here to really honor that gift and we’re so appreciative of being able to share that space with them and being able to hopefully provide a little bit of brightness in a very dark time.”




